The erection process is to be understood as a neurally controlled, hemodynamic event, which is influenced by an intact hormonal situation and an adequate mental state [12]. As a cerebral sexual center, the limbic system localized in the temporal lobe is considered to be of the greatest importance. Erectile stimulation triggered by the cerebrum paves its way via the thoracolumbar center Th L1-L3 (= psychogenic erectile center), which delivers efferent sympathetic fibers via the border ganglia to the superior and inferior hypogastric plexus. Parasympathetic influxes are received by the inferior hypogastric plexus from sacral segments S2-S4 (= reflexogenic erectile center) via the erigent nerve. The efferent-parasympathetic fibers reach their terminal organ via the pudendal nerve, the sympathetic-efferent fibers periarterially in the corpus cavernosum.
In the resting state, according to current ideas [11], the penis is under a sympathetic tonic permanent vasoconstrictor tone and probably under the modulating influence of local neuro-effectors such as the “vasoactive intestinal polypeptide” (VIP) and in equilibrium with cholinergic neurotransmitters responsible for the control of corporal muscle relaxation. Triggering of the erectile process via relaxation of sympathetically toned cavernosal muscles is most likely the blockade of sympathetic impulses, although the transmitter for this process is still unknown. Parasympathetic cholinergic neurotransmission also appears to be mediated by an endothelium-derived relaxing factor (EDRF) secreted by the endothelial cell, with a local increase in nitric oxide (NO) thought to support the development of EDRF's effects [10]. Adrenergic, cholinergic, and VIP-ergic neurostimulation are thus interrelated in a way that is not yet fully understood [1-4, 6, 9].
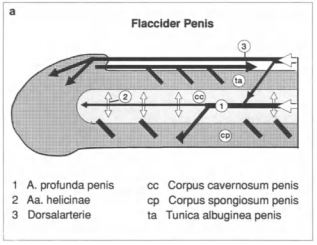
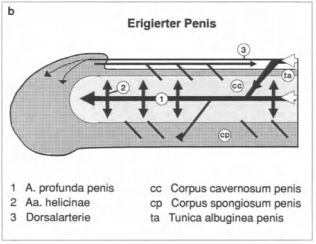
Fig. 1.3 a, b. Schematic representation of arterial inflow and venous outflow conditions during erection.
In the resting state (flaccid penis), the intracorporeal arterioles are constricted and the smooth corpus cavernosum muscles are contracted, so that the blood inflow via the profunda artery and, to a lesser extent, via the dorsalis artery is in balance with the free blood outflow via the emissary veins at the level of the corpus cavernosum (fig. 1.3). The following hemodynamic components are responsible for the tumescent and erectile phases (Fig. 1.4 a, b):
Initial evidence also suggests additional active restriction of venous outflow tracts as an additional veno-occlusive mechanism [7].
The greatly reduced venous blood outflow with a massive increase in arterial inflow and the additional compression of the tumescent corpus cavernosum by contraction of the ischiocavernosi and bulbospongiosi muscles lead to maximum rigidity. In the detumescent phase, increased venous outflow occurs with decreased arterial inflow [5]. Figure 1.5 is a simplified representation of the hemodynamic processes.