An orally available medication for the therapy of erectile dysfunction is, according to reports from the literature and experiences with our patients, the preferred treatment alternative for most affected persons. Compared to other methods, this method is characterized by the fact that spontaneity of sexuality is not impaired and that this therapy is not necessarily revealed to the partner (as is the case, for example, with SKAT or the use of a vacuum system). Furthermore, possible side effects such as hypotonia or a stuffy nose seem more acceptable to many patients than a prolonged erection or cavernous fibrosis with consecutive penile deviation after SKAT.
Although reconstructive surgery and prosthetic fitting are — in principle — methods available that also allow spontaneous sexuality, these options should only be used very selectively due to their much higher invasiveness and uncertain prospects of success (reconstructive surgery) or irreversible destruction of the cavernous tissue (prosthesis).
Basically, oral agents for the treatment of erectile dysfunction can currently be divided into 2 different groups, depending on the mechanism of action (see overview). On the one hand, there are substances with a central point of action, such as yohimbine, apomorphine, trazodone, or newer serotonin reuptake inhibitors (SSRIs); on the other hand, there are drugs with peripheral effects, such as phentolamine or sildenafil (which probably also has a central effect).
Overview 1: Targets of orally active substances:
Yohimbine (Yohimbine “Mirror” or “Yocon”) is the only orally active substance currently approved for the treatment of erectile dysfunction. Since the registration of this active substance was still carried out with documentation material that no longer meets today's approval criteria, a follow-up approval must now be obtained, as is the case with many other drugs, with studies that are now accepted as standard; these will be completed shortly. If these prospective, placebo-controlled studies are positive, yohimbine will continue to be available for the oral treatment of erectile dysfunction.
Yohimbine was isolated from the bark of a tree native to Central Africa (Corynanthe yohimbe K. Schum.), which is still used today as a starting material for the production of the drug yohimbine HCL. Double-blind, placebo-controlled studies regarding the efficacy of the substance in erectile dysfunction can be found in the literature [6, 8, 9, 11, 13]. In these studies, as well as in our patients [3], it was shown that the indication for yohimbine therapy is crucial for success: while administration in unselected patients led to a significant improvement in erectile response in only a marginal percentage, satisfactory results were obtained in patients with predominantly psychogenic or borderline organogenic findings.
In terms of side effects, mainly rather minor phenomena were observed, such as restlessness of various degrees, hand tremors, nasal congestion, and sleep disturbances. While blood pressure increases have occasionally been reported in the literature following yohimbine, our experience shows the opposite, namely a reduction in blood pressure. Since a conclusive judgment is obviously not possible here, blood pressure should be checked at follow-up appointments; these appointments should be appropriately close in patients at risk.
In the absence of side effects, the following dosage has been found to be recommended: During the first 3 days of intake, 3 times 5 mg is prescribed, which is then increased to 3 times 10 mg maintenance dose. The patient should be informed in advance that an onset of action usually occurs only after about 14 days and that the intake should be carried out for at least 6 weeks.
Apomorphine acts as a dopamine receptor agonist and at p-, 6- and K-receptors of the central nervous system. Heaton et al [4] observed that when 4 and 6 mg of apomorphine were administered in a sublingually administrable form, a positive effect on erectile function was observed at a dosage at which vomiting was still absent in a large proportion of patients. In patients with probable psychogenic erectile dysfunction, a GV-capable erection under RigiScan control or home conditions following apomorphine was reported in over 70% of cases [4]. Although the mechanism of action appears attractive and these initial results indicate a positive trend, with a placebo rate of approximately 40% and relatively few patients overall, a larger study, including organogenic patients, must be awaited before the potential of this compound can be assessed.
Trazodone is a triazole pyridine with, among other things, serotonin reuptake inhibitor activity and is widely used clinically as an antidepressant. In this indication, increased erectile activity and prolonged erections have been frequently reported as side effects in the literature [10]. However, in a prospective, placebo-controlled study in patients with erectile dysfunction, no better therapeutic effect than placebo was observed [5], so that its use in this indication (outside controlled studies) cannot be advocated at present.
Phentolamine is a non-selective a-receptor blocker that has been used for several decades in various indications. Zorgniotti, Gwinup and Wagner each reported on different studies in which sublingually administered phentolamine led to a significant improvement in erectile function. In a prospective, placebo-controlled study, we also found a significant improvement in erectile function after a single dose of rapidly absorbable phentolamine in 40 patients with organogenic erectile dysfunction at our center [12], while the results of the overall study (n = 177) were not significantly different from placebo [7]. Here, it remains to be seen what further currently ongoing studies in America will reveal. In principle (if it proves to be effective), a further oral therapy option with a substance that has already demonstrated great drug safety in humans over decades would be welcome.
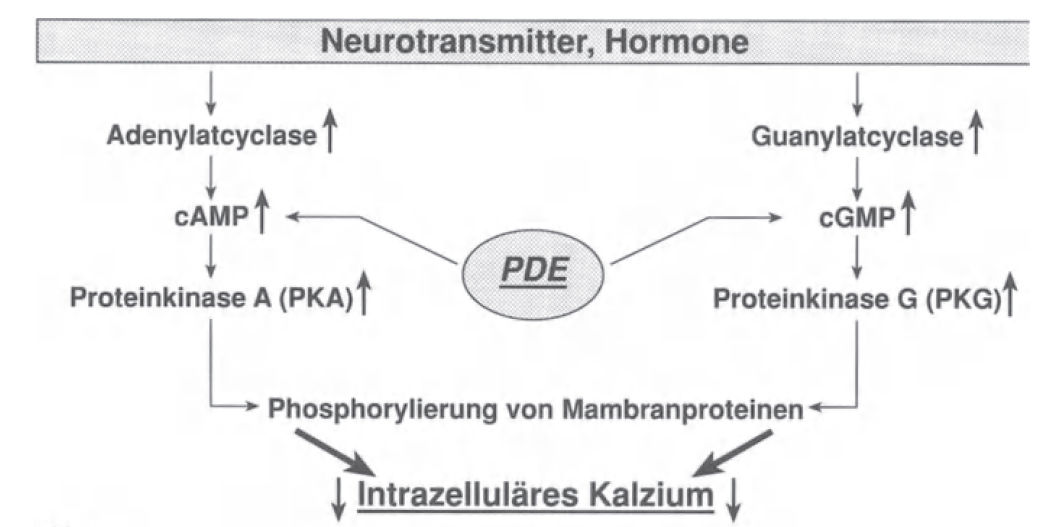
Sildenafil is a selective inhibitor of phosphodiesterase V, an intracellular enzyme that degrades the cyclic nucleotides cAMP and (especially) cGMP. Inhibition of this phosphodiesterase (PDE) results in an increase in intracellular messengers, which then leads to smooth muscle cell relaxation via a complex cascade (Fig. 2.1). Initial results [1, 2] showed strong efficacy of orally administered sildenafil in patients with psychogenic erectile dysfunction. In principle, the mechanism of action of sildenafil is attractive, although initial euphoric response rates of 88% appear far excessive. Furthermore, due to the presence of PDE V in the brain, an additional central component of sildenafil can be postulated. Overall, the currently available data from controlled trials suggest that this mechanism of action will provide an attractive therapeutic option for the treatment of erectile dysfunction.