Angiographic imaging of the penile vessels is an invasive, technically complex radiological diagnostic procedure whose use is no longer justified for purely diagnostic purposes. Ultrasonographic procedures, in particular color-coded duplex sonography, provide the patient with risk-free functional parameters in addition to morphological information, which cannot be obtained from angiography. Nevertheless, there are still indications for this examination in the context of expert opinions, especially in cases of post-traumatic erectile dysfunction [2] (see Chapter 13), but also in cases of suspected vascular malformation in the pelvic region as a possible cause of erectile dysfunction. Various research groups perform angiography even before revascularization surgery of the penile vessels; again, this does not appear to be mandatory, since penile anastomoses are performed almost exclusively. If dilatation of the iliac artery is considered as a therapeutic route, angiography is indispensable. Of course, the indication for survey aortography remains unaffected if disorders in this area are suspected, but in which erectile dysfunction is only an additional symptom, such as in Leriche syndrome (chronic ischemia of the lower extremities associated with erectile dysfunction). Visualization of the iliac artery additionally allows visualization of the inferior epigastric artery (Fig. 3.7), the integrity of which is a prerequisite for an epigastricopenile anastomosis. This examination should be requested especially if the patient has previous operations in the lower abdomen to avoid unnecessary epigastric exposure. As with sonographic procedures, arteriography of the penile vessels is worthless without the use of vasoactive substances as part of the SKAT test to assess penile vascular changes (Fig.3.8).
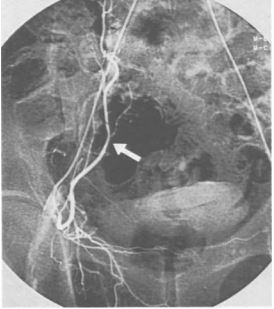
Fig. 3.7. Strong inferior epigastric artery suitable for epigastricopenile anastomosis (arrow).
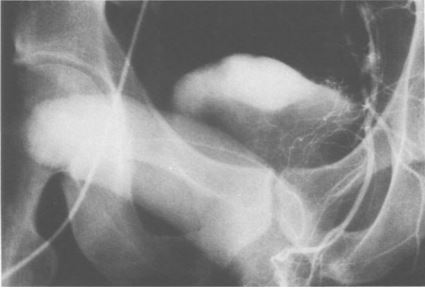
Fig. 3.8. Illustration of the right dorsal and profunda penis arteries (normal findings).
With the patient in the supine position, after puncture of the femoral artery in the inguinal region, if at all necessary, a survey view of the aortic bifurcation is performed (Seldinger technique). Subsequently, the internal iliac artery is selectively catheterized. A schematic representation of the penile arterial supply is given in Fig. 3.9. For selective catheterization of both internal pudendal arteries as terminal branches of the internal iliac artery, a cross-over technique is generally necessary, i.e., the right pudendal artery is probed by the left femoral artery and vice versa (2 punctures!).
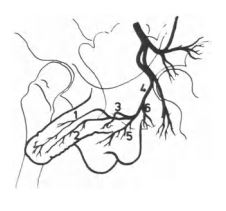
Fig. 3.9. Schematic representation of the branches of the internal iliac artery. 1, A. dorsalis penis; 2, A. penis profunda; 3, A. bulbaris penis; 4, A. pudenda interna; 5, A. perineal superficialis; 6, A. rectalis interior.
After probing the internal pudendal artery, the vasoactive substance is applied intracavernosally and its effect is waited for 5-10 min before the actual imaging of the penile vessels is performed (Fig. 3.8). The examination can be performed under local anesthesia, although vasospasm is more likely to be avoided with peridural anesthesia, resulting in better quality images. Here, the limit of reasonableness for the patient is touched. If a surgical procedure is planned, the outflow and course of the inferior epigastric artery should be visualized. Conventional large-blade angiography technique and digital subtraction angiography are used as technical procedures, with the latter procedure having a lower radiation exposure.
Local complications potentially occurring at the puncture site include: Hematoma formation, thrombosis, embolism, vessel dissection, aneurysm formation, arteriovenous fistula formation, infection, and rebleeding from the puncture site. Systemic side effects are primarily due to contrast agent application in the sense of a hypersensitivity reaction, which have become very rare with the use of nonionic contrast agents. In addition, radiation exposure must be considered, which is why patients with ongoing family planning are advised to refrain from fathering a child for six months [1]. Contraindications to angiography include severe contrast allergy, renal insufficiency, or blood clotting disorders.
Because primary impotence must be suspected to be a congenital vascular malformation that may not be diagnosed on Doppler sonographic examination, the indication for angiography should be more generous. Vascular angiomas [3], arteriovenous fistulas [4], and hypoplasias have been described as such malformations [1]. Whether unilateral hypoplasias are really the cause of erectile dysfunction or just an incidental finding is often difficult to decide in individual cases.
Although high correlations between penile angiography and Doppler ultrasonography have been described, Doppler ultrasonography has the higher value in the penile area, so that pathological angiographic findings should be checked here. In secondary impotence, angiography is still important, especially in post-traumatic erectile dysfunction, in the context of expert opinions on the localization and extent of the injury. Traumatic AV fistulas can also only be diagnosed in this way. However, the hemodynamic relevance of described morphological changes can only be determined by Doppler ultrasonography.
Penile angiography is an invasive examination procedure to detect pathological changes in the internal iliac artery and penile vessels. In the routine screening of patients with erectile dysfunction, this method has been superseded by ultrasound-guided procedures and remains reserved for a few selected indications because of the technical complexity and potential risks to the patient.