Diseases of the corpus cavernosum with a possible negative influence on erection include induratio penis plastica, local enamel body damage after trauma or diseases without an identifiable cause, but also damage resulting from treated or untreated priapism. Congenital or acquired penile deviations can also lead to cohabitation disorders and are described in a separate chapter (Section 10.1.3).
Induratio penis plastica is a disease associated with connective tissue proliferation in the area of the tunica albuginea. The cause of this disease is unclear, a connection with trauma is not seen. The disease is also known to spread to the corpus cavernosum, characterized sonographically by microcalcifications in the corpus cavernosum. Anamnestically, patients report penile deviations, mostly dorsal, which may lead to cohabitation difficulties. On clinical examination, palpable nodular formations are often found in the tunica albuginea region. If induratio penis plastica coincides with erectile dysfunction, the underlying cause is usually a venous occlusion disorder (Fig. 4.3). If there is no response to intracavernosal injections, which may well be the case in individual cases, penile prosthesis implantation is an alternative therapy. In individual cases, reconstructive surgery by combining penile rectal surgery with resector vein surgery may also be indicated. (For further details on the therapy of induratio penis plastica, see Chap. 10.1.3).
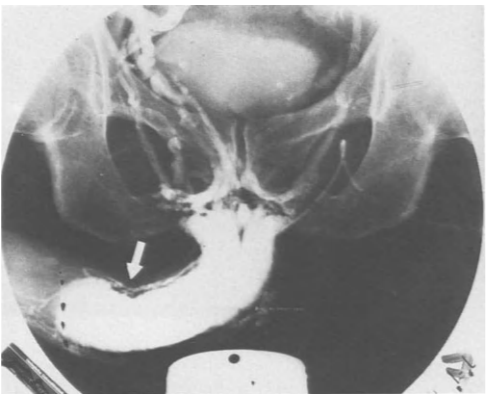
Fig. 4.3. Pharmacocavernosogram of a patient with induratio penis plastica and erectile dysfunction due to venous occlusion disorder. Plaque indicated by arrow.
Priapism is a continuous excitation that is not induced by sexual stimulation and cannot be interrupted voluntarily. In the vast majority of cases, the cause remains unclear (idiopathic priapism). Priapism can occur in hematological or malignant diseases, but also in inflammatory diseases, especially of the CNS (Lues!) or induced by medication. The most common form of priapism is stasis priapism, characterized by complete cessation of blood flow in the corpus cavernosum. The timing of treatment is of critical importance. After 24 hours, irreversible damage to the corpus cavernosum can be expected (Fig. 4.4). The most common surgical procedures are the formation of a glandulocavernosal shunt according to Winter and anastomosis of the great saphenous vein with the corpus cavernosum according to Grayhack. In the rare form of high-flow priapism (Doppler sonographically preserved flow in the profunda vessels, cavernosographically persistent venous outflow), reversible embolization of the internal pudendal artery with blood clots performed in the Seldinger technique is also successfully used. Drug treatment of prolonged erection is presented in chap. 9.
Erectile impotence is, along with urethral stricture (Fig. 4.5) and urinary incontinence, the most important late complication of posterior urethral rupture, which usually occurs as a result of pelvic fracture. The frequency of occurrence of partial or complete loss of erectile function is reported in the literature to be between 3011.10 and 60% of cases [21]. Spontaneous improvement is still reported to be possible in a period of up to 4 years. However, primary conservative treatment of urethral rupture by cystostomy and catheter splinting of the anastomosis improved the postoperative impotence rate. Compared with surgical revision with primary urethral suturing, impotence rates below 10,070 have been published with this procedure. However, in addition to the treatment strategy, the trauma itself has causal significance in the development of erectile dysfunction. In particular, occlusions of the internal pudendal artery (Fig. 4.6) represent a frequent concomitant injury of urethral ruptures. However, nervous involvement in the sense of impairment of the pudendal nerves can also be objectified based on pathologic bulbocavernosal reflex latency measurements (see Chap. 5). The unremarkable neurological examination in the presence of pathological arterial inflow (Doppler, angiography!) and the absence of occlusive disorder are favorable prerequisites for revascularization surgery of the penile vessels in younger patients. In addition, it should be mentioned that blunt trauma of the pelvis or perineum due to injury of the pudendal vessels may also be the cause of erectile dysfunction [12]. At the same time, it is suggested that blunt trauma to the pelvis or perineum may be a potential risk factor for the subsequent development of arterial-vascular erectile dysfunction [12].
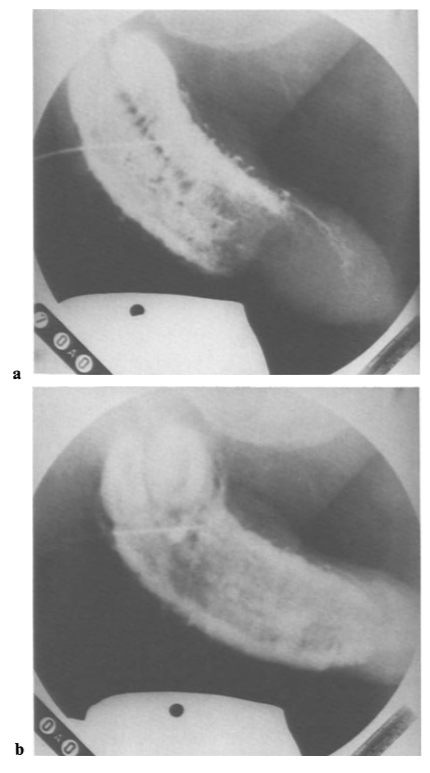
Fig. 4.5 a, b. “Artificial cavernosogram” in the case of high-grade urethral structure in the micturition cystourethrogram (filling of the urinary bladder via suprapubic catheter with contrast medium). a) Visualization of the posterior urethra up to the bulbar, b) staining of the entire cavernous body by transfer of contrast medium from the urinary tube.
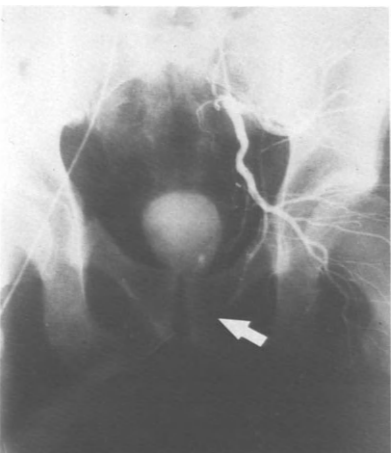
Fig. 4.6. Selective visualization of the internal iliac artery without staining of the penile vessels in a 40-year-old patient after pelvic ring fracture and urethral avulsion (discontinuation of contrast marked with arrow).