Inspection and palpation of the external genitalia are used to detect congenital or acquired malformations and testicular consistency. Testicular size should be determined by orchidometer, with volumes <15ml classified as atrophy. If no testes are palpable in the scrotum, congenital anorchia may be present, additionally characterized by the absence of secondary sexual characteristics and an eunuchoid habitus. Differentially, a maldescensus testis on both sides must be considered, and further diagnostic measures must be initiated if necessary (Fig. 2.1). Clinically far more common is Klinefelter syndrome, characterized by gynecomastia, female pelvis, tall stature, small testes, and azoospermia. The cause of the syndrome is a chromosomal abnormality (XXY).
In patients who usually consult the andrology department because of infertility, a testosterone deficit may develop due to increasing Leydig cell insufficiency, which clinically leads to impotence. An estrogen-producing tumor (e.g., Leydig cell tumor), which may be clinically noticeable not only by gynecomastia but also by a decrease in libido, is typically detectable as a local hardening on testicular palpation. Palpation of the corpus cavernosum can provide evidence of induratio penis plastica, which is frequently clinically associated with limb curvature, by detecting local hardening. In contrast, congenital deviations of the penis, which can also lead to cohabitation disorders, do not show any hardening of the tunica albuginea and can only be proven by erection provocation with an appropriate medical history. The examination concludes with rectal digital examination of the prostate. Painful, doughy consistency is found in bacterial prostatitis, but also in neurovegetative prostatopathy, in which ultimately no consistent organic pathologic finding can be elicited. An overview of the clinical andrological examination is given in Table 2.4.
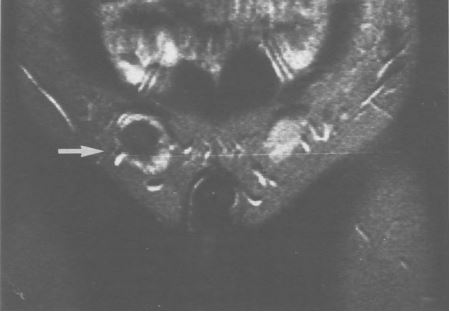
Fig. 2.1 Magnetic resonance image showing maldescensus testis is on both sides in a 24-year-old patient, right inguinal testis enlarged and low in signal (later histology: malignant teratoma).
Table 2.4 Clinical andrological examination.
The clinical andrological examination is used to detect diseases of the external genitalia that may be involved in erectile dysfunction. The constitutional habitus gives clues to a possible disorder in connection with the sex hormones.