Further investigation methods are currently being carried out primarily from a scientific perspective. A relevance for current use in practice can therefore not yet be conclusively assessed.
The initial favorable results in the visualization of changes in the tunica albuginea in induratio penis plastica using STS were described by Austoni et al. [1] (Fig. 3.14). However, in this disease, information about the extent of changes in the corpus cavernosum can be obtained more quickly and cost-effectively employing corpus cavernosum personography according to SKAT. Sohn [6] reported the distribution pattern of the STS contrast agent gadolinium-DTPA (Magnevist) within the corpus cavernosum as a possible investigative method to assess the arterial supply to the corpus cavernosum. Overall, a conclusive indication for this procedure in the penile area cannot be made at this time. However, MRI represents the most important diagnostic method for the detection and localization of pituitary prolactinomas as a cause of erectile dysfunction and has displaced the X-ray sella image regarding this indication.
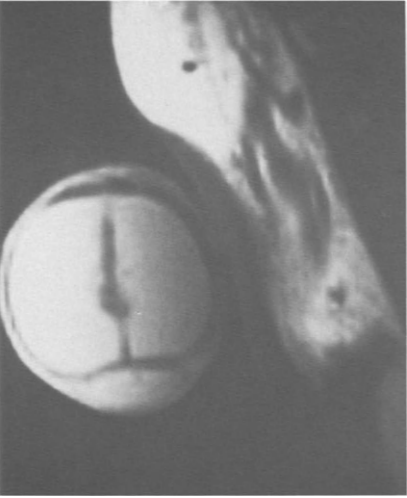
Fig. 3.14. Magnetic resonance imaging of increased connective tissue structures in the region of the corpus cavernosum in induratio penis plastica.
Intravenous application of a radionuclide (99mTc-pertechnetate) has been used to visualize hemodynamic changes during erection as a screening method to objectify arterial changes [4]. Washout of subcutaneously applied 133Xe [2], sometimes after intracavernosal injection of Prostaglandin Ej, has also been used for clinical and scientific purposes. Due to controversial results, this method has not yet found its way into routine diagnostics.
A possible coincidence between erectile dysfunction and bladder voiding dysfunction, which is found more frequently in neurogenic diseases and after radical pelvic surgery, can be explained by the common nerve supply to the urinary bladder and the corpora cavernosa via parasympathetic branches of the pelvic nerve and sympathetic fibers of the hypogastric nerve. In the case of a conspicuous micturition history, an urodynamic examination with simultaneous videographic recording can offer help in detecting vegetative neuropathies in the pelvic region. In this examination, the urinary bladder is filled with warm (37 DC) contrast medium with the aid of a transurethrally or suprapubically inserted double-barrel catheter (8 Charriere) and the bladder pressure is measured simultaneously. Abdominal pressure is measured via a fluid-filled balloon probe in the rectum.
A multichannel recorder continuously records bladder filling volume, micturition volume, urine flow and possibly the electromyogram of the pelvic floor. Detrusor pressure, defined as the differential pressure of intravesical and rectal pressure, is calculated electronically utilizing a subtraction amplifier and is also recorded continuously. In particular, simultaneous videourodynamics allows the urodynamic parameters to be correlated simultaneously with the morphological abnormalities of the urinary bladder. It is this type of examination that allows a more precise analysis of confounding factors, which is not possible with conventional urodynamics. An example is partial paralysis of the urinary bladder wall, which is considered a direct indication of partial neurological impairment of urinary bladder innervation (e.g., postoperative or post-traumatic neuropathy). These findings may become particularly important in the evaluation of post-traumatic erectile dysfunction when combined with micturition disorders.
The recording of electrical potentials via needle electrodes inserted into the corpus cavernosum has been presented as a possible diagnostic method for the detection of neuropathy of autonomic corpus cavernosum innervation and for the diagnosis of cavernous myopathy [7]. Desynchronization of electrical potentials is thought to be indicative of autonomic neuropathy, whereas low amplitude and slow depolarization are indicative of cavernous myopathy. Although the method seems to provide reproducible results, the origin of the derived potentials is unclear. An etiologic assignment of the collected “pathologic” findings to clinical findings seems premature at present and needs further scientific investigation.
Although changes have been found in arterial and combined arterial-venous erectile dysfunction using electron microscopy, particularly in the area of smooth cavernous muscle cells [5], light microscopic morphological examination of the erectile tissue biopsy specimen cannot currently contribute to the pathological clarification of erectile dysfunction and cannot yet be recommended as a diagnostic measure [3]. Further research is currently underway in this area.