Whereas with CW-Doppler, the signals of neighboring vessels lying in the same sound cone cannot be distinguished from each other, the duplex system, also known as pulsed Doppler, allows exact velocity measurement in a sonographically adjusted vessel section. The advantages of these devices are thus obvious. In addition to velocity measurements in the vessel, an analysis of the pulse curve is possible (Fig. 3.1). This examination is also only useful in the context of the SKAT test, whose central importance for diagnostics is again emphasized [3]. Sound frequencies of at least 7.5 MHz or more are useful for penile duplex sonography in this context. Characteristics of the healthy vessel are strong vessel pulsations (however, already recognizable in the B-scan), a vessel diameter of 1 mm after injection, and a maximum velocity above 25 cm/sec [5] (Fig.3.2). A disadvantage for conventional devices is the poor detectability of the dorsalis penis artery. Furthermore, measuring vessel velocity alone without considering vessel morphology can lead to misinterpretation, as high velocities are often measured, especially in the area of stenosis. A vessel obstructed proximal to the corpus cavernosum, on the other hand, may show sufficient drug-induced dilatation, with only low air velocities found. Thus, both criteria, the dilatability of a vessel and the measured blood flight velocity, must be included in the evaluation of vascular function. With conventional duplex sonography, soft tissues and the vessel lumen can be imaged, but only an orienting overview of the blood flow can be obtained, since the measurement of the frequency shift is only possible at one point within the B-scan. It is not possible to record the blood flow over the entire image area and especially of smaller vessels with this method.
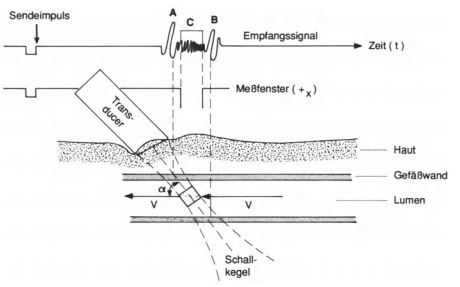
Fig. 3.1. Principle of duplex sonography (from [4]).
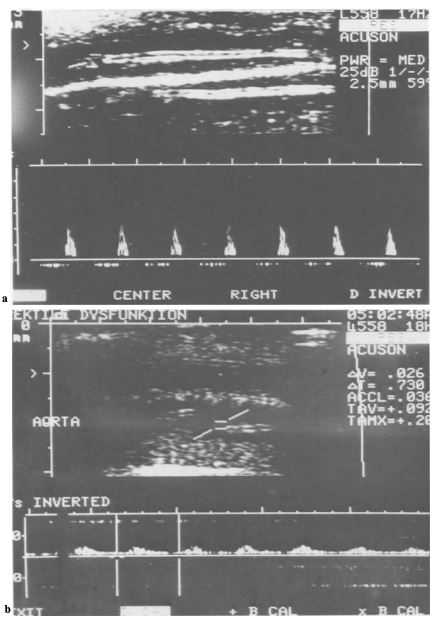
Fig. 3.2 a, b. Conventional duplex sonography (cursor in a profundal artery). a) normal findings, b) arteriopathy.
In color-coded duplex sonography, a further development of duplex sonography, the image of the blood flow is color-coded on top of the gray-scale image. The ultrasound signals back-scattered by the moving blood cells are color-coded as a function of their direction of motion and velocity. Dorsal and profundal vessels are thus visible over the entire image area, whereas with conventional duplex systems the blood flow can only be measured at a single point. The magnitude of the frequency shift is represented by the intensity of the color and the direction of the blood flow by two different colors (red and blue). For example, a fast flow of blood toward the transducer is shown in light red, while a slow flow away from the transducer is shown in dark blue. This allows flow direction and flow velocity to be qualitatively assessed. Due to the different color saturation in the image, a semi-quantitative statement about blood supply and blood flow velocity is immediately possible (Fig.3.3).
The clinical examinations of patients with erectile dysfunction with suspected arterial genesis proved that the localization and extent of vascular stenoses of the penile arteries can be visualized in the sonographically accessible areas of the corpus cavernosum. Simultaneous visualization of morphological changes (stenosis, occlusion) and imaging of functional parameters (turbulence and increased flow velocity in the stenosed area) allow criteria of vascular damage to be visualized in a way that is not possible with any other imaging technique. For the first time, it was possible to gain insight into the supply of peripheral corpus cavernosum areas by imaging the helicine arteries. Colored blood imaging revealed abnormal intracorporeal supply patterns [1] in penile arterial vasculopathy (Fig. 3.4). However, the method is limited to the penile region. Vascular changes in the pelvic region as a possible cause of arterial erectile dysfunction can be clearly visualized only with angiography. The visualization of vascular anomalies, such as unilateral erectile arterialization from the dorsalis penis artery (Fig. 3.5), was achieved for the first time with this procedure. However, especially in the presence of vascular malformations, the procedure can only describe the findings. Whether the anomaly is only a norm variant or the cause of the clinically indicated erectile dysfunction cannot always be decided based on the image findings and the measurement parameters. Devices with a special “slow-flow option” make flow measurements in the dorsalis penis profunda possible in addition to penile arterial flow measurements. However, since in so-called “venous insufficiency” the cavernosal function is crucial, this method will not be able to replace cavernosometry and cavernosography.
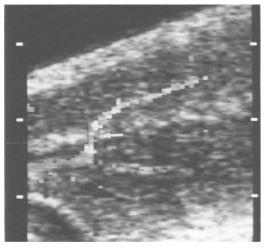
Fig. 3.4 Arterialization of a cavernous artery from the contralateral artery through the cavernous septum (arrow) in proximal stenosis.

Fig. 3.5 Arterialization of a corpus cavernosum from the dorsal artery (vascular malformation).
Fig. 3.6. Increasing performance of various doppler sonographic systems.
Duplex ultrasound devices, in conjunction with the SKAT test, currently represent the most powerful diagnostic method for detecting penile arterial vasculopathy. Color-coded ultrasound devices are superior to conventional devices due to better visualization of penile vascular anatomy.